Panorama 22q11 test

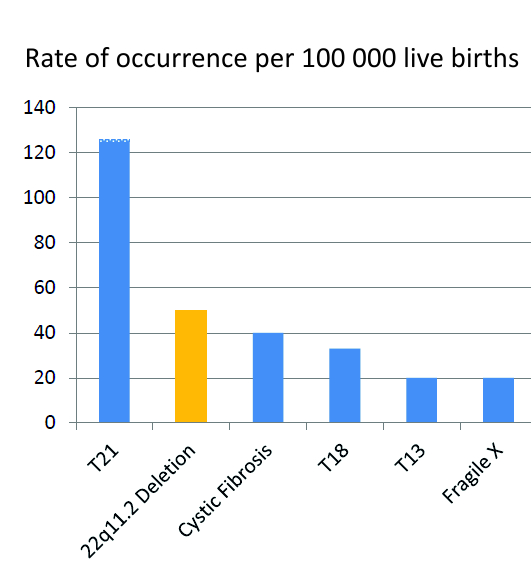
About one in 2000-4000 live births experiences 22q11.2 deletion syndrome, which could cause several congenital disorders and also an average to moderate mental disorder.
22q11.2 is one of the most common causes of developmental disorders and congenital heart diseases, only slightly less than Down syndrome. These syndromes are similar, as both have many disease symptoms, including low muscle tone.
What is 22q11.2 deletion syndrome?
22q11.2 deletion syndrome, i.e. DiGeorge syndrome, is caused by the absence of a small piece of the arm of the 22nd chromosome.
.jpg)
The resulting condition has an impact on a significant part of the body. Most of the children with the syndrome have heart failures, immune disorders and specific, although hardly noticeable, features. Almost all of them have average to moderate disorders and delayed language and speech development. Some children have a lack of calcium, kidney problems, eating problems, cramps or other health problems. Approximately one out of five children with 22q11.2 deletion syndrome has autism spectrum disorder, and one out of four young adults suffers from a psychiatric disorder, such as schizophrenia. The infants with severe heart problems or immune system disorders have a higher risk of dying. The people with 22q11.2 deletion syndrome who survived their childhood could have a shorter lifetime and a higher risk of sudden death.
What is the reason for 22q11.2 deletion syndrome?
Most people with 22q11.2 deletion syndrome have a 3 MB deletion (involving an average of 40 genes) on one copy of the 22nd chromosome. 22q11.2 deletion is occasional and is mostly not hereditary. However, approximately 7% of the children with the syndrome, as is known, inherited this from their parents, who were sick with the same condition. The testing of both parents could help to determine the likelihood of recurrence of such a condition in the case of the next pregnancy.
Why is the diagnosis of 22q11.2 deletion syndrome important?
The treatment of conditions listed below, as well as the combination of physiotherapy, work therapy, and special training, could improve patients' quality of life with 22q11.2 deletion syndrome.
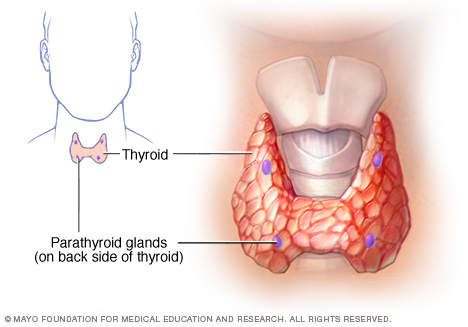
- Hypocalcemia. Low levels of calcium, i.e. hypocalcemia, are common in the case of 22q11.2 deletion syndrome, foremost in newborns. This is due to the deficient functioning of the thyroid glands. The lack of calcium caused by parathyroid hormone deficiency could result in cramps. The reasons for cramps caused by the low calcium level are often left unattended. Thus, the problem could remain without treatment and influence the child's mental development. The newborns with 22q11.2 deletion syndrome should be observed for the signs of hypocalcemia, and if these are established, the child should be immediately treated. Hypocalcemia could recur during growth spurts, puberty or during illness and pursuant to the operations.
- Immunodeficiency
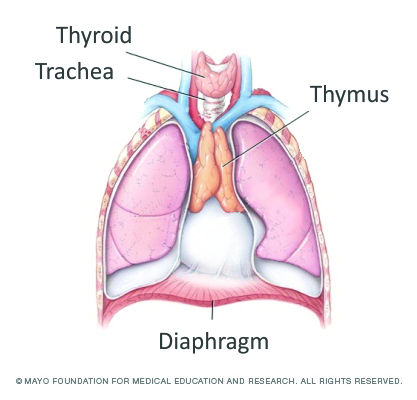
The lymphatic system is an important part of the immune system, which protects a child against infections. The parts of the lymphatic system are the spleen, thymus, lymph nodes and vessels, tonsils and adenoids. About 75% of the children with 22q11.2 deletion syndrome have immunodeficiency. Due to the risk of immunodeficiency, the children with the syndrome should be checked prior to taking live virus vaccines.
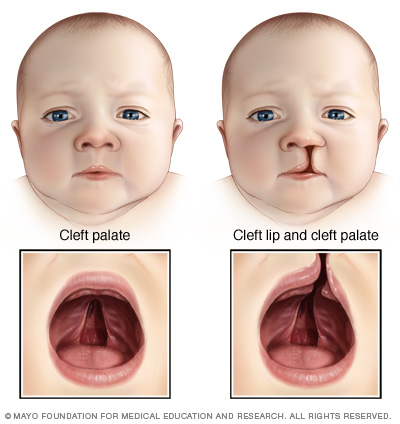
- Palate malformations. Approximately 75% of the children suffering from the syndrome have a palate problem, which is either structural or functional, or a combination of both. This problem could cause eating difficulties and/or speech disorders. If the problem is not fixed in good time, it could influence the development of speech. Such a condition can be mostly treated.
- Eating difficulties. The newborns with 22q11.2 deletion syndrome often have eating difficulties which are not caused by the palate or heart failures. The reason for eating difficulty could be motor disorders of the pharynx and larynx muscles, the most common symptoms of which are reflux and constipation. The intestinal malrotation and Hirschsprung’s disease could seldom occur. Most of these problems can be treated.
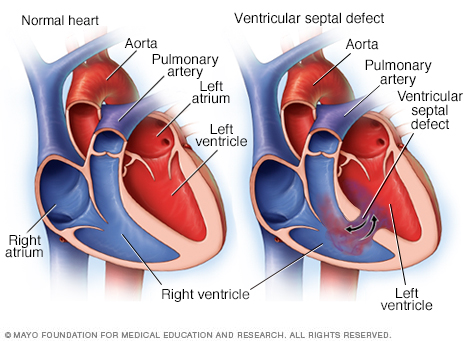
- Congenital heart failures. Approximately 75% of the people with the syndrome have congenital heart failure; such an indicator is often the basis for diagnosing the syndrome. If 22q11.2 deletion syndrome is diagnosed for the patient, he/she should be referred to a cardiologist for evaluation. Many heart failures are operable today.
- 22q11.2 deletion syndrome also involves other medical problems, including kidney problems, loss of hearing, ear-nose-throat complications, autoimmune diseases, growth retention and skeletal system problems.
How should I relate the high-risk result of the Panorama test to 22q11.2 deletion syndrome?
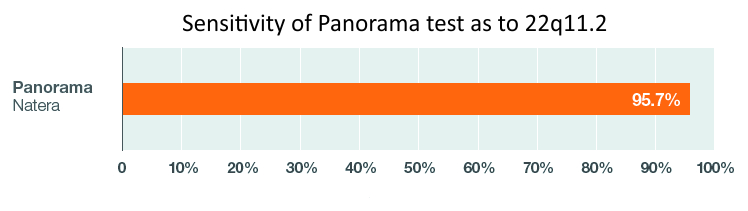
The sensitivity of the Panorama test in detecting 22q11.2 microdeletion is 95.7%, and the specificity is > 99%. Thus, this is an accurate screening test.
However, regardless of the accuracy, the Panorama test will still be a screening test. Without the ultrasound markers, the estimated positive value of the Panorama test is only 20%. At the same time, in case of positive ultrasound findings (heart failure, small thymus), the estimated positive value of Panorama is close to 100%. Thus, this is not a diagnostic test. In case of a Panorama test with high risk, the amniotic fluid test or chorion biopsy confirming the diagnosis should be performed. This also involves submicroscopic chromosome analysis, which can detect the missing piece of the 22nd chromosome causing 22q11.2 deletion syndrome. If a woman does not require an invasive test during pregnancy, the chromosomes received from the vein blood of the newborn after birth could be examined with the help of submicroscopic chromosome analysis.
The estimated negative value of the Panorama test for 22q11.2 is 99.9%. Thus, the possibility that the Panorama test does not recognise the disease is very low.
The sensitivity of the Panorama test in detecting DiGeorge syndrome depends on the amount of cell-free fetal DNA. If the amount of cell-free fetal DNA by screening negative women is higher than 6.5%, the fetal risk under the 22q11.2 microdeletion test is 1:9000 per one birth, which could be considered very reassuring.
Can 22q11.2 syndrome be tested also in case of twin pregnancy?
22q11.2 syndrome can be tested only in monochorionic twins (twins sharing one placenta and are always monozygotic twins). 22q11.2 syndrome could not be tested in case of dichorionic twins (twins having their placenta and could be either monozygotic or dizygotic twins) and in case of IVF pregnancy, provided donor eggs have been used.
DiGeorge syndrome could not be tested in case of dichorial twins (twins who both have their placenta and could be either monozygotic or dizygotic twins) and in case of IVF pregnancy, if egg donors have been used.
Panorama test + DiGeorge test is not performed:
- If the pregnancy is less than 9 weeks
- If the fetus has a developmental defect detected by ultrasound or if NT > 3.0 mm*
- If one of the fetuses has vanished in a twin pregnancy.
- For twin pregnancy, if the mother has dichorial twins (dizygotic twins)
- In the case of IVF pregnancy, when the mother has become pregnant using a donor egg**
- For triplets
- If the pregnant woman has had a bone marrow transplant before pregnancy
- If the mother has been previously diagnosed with DiGeorge syndrome.
* If the fetus has a developmental defect detected by ultrasound or if NT is > 3.0 mm, we recommend a chorionic villus sampling, because the Panorama 22q11.2 test cannot detect all genetic and chromosomal diseases that may occur in the fetus with an increased NT.
** In cases of IVF pregnancies where the mother has used a donor egg, the Prenatalsafe KaryoPlus test can be utilised instead.