Preeclampsia Screening During Pregnancy – How Loote Ultrahelikeskus Can Help You

May has been designated by ISUOG to raise awareness of preeclampsia, its risks, and the potential for early detection.
Pregnancy does not always progress as calmly and smoothly as we hope in the beginning. One of the reasons women come to our clinic is high blood pressure during pregnancy, previous preeclampsia, or fear of developing this condition.
Preeclampsia is one of the most common pregnancy-related hypertensive disorders and may affect both the mother and the unborn baby.
Receiving such a risk assessment or diagnosis may raise many questions.
- Is my baby developing normally?
- Is the placenta functioning properly?
- Could my pregnancy become dangerous?
- What happens next?
I would like to reassure women that they are not alone with this concern.
An increased risk of preeclampsia does not mean that something has gone wrong. It simply means that your pregnancy requires closer and more personalized monitoring.
As a fetal medicine specialist, my most important question is not whether the mother’s blood pressure is normal today. The most important question is how the placenta is functioning and how the baby is growing.
Preeclampsia usually does not appear overnight. In many cases, changes in placental development begin very early in pregnancy, long before high blood pressure or clinical symptoms appear.
That is why, at Loote Ultrahelikeskus, we always try to think several steps ahead.
What is preeclampsia screening?
Modern preeclampsia screening helps assess the risk of pregnancy-related hypertension, placental insufficiency, and fetal growth restriction already in early pregnancy.
Preeclampsia screening is not based only on individual risk factors or maternal history. Risk is calculated using a specialized algorithm that combines:
- maternal medical and obstetric history
- standardized blood pressure measurement
- uterine artery Doppler examination
- biochemical placental markers (PlGF and/or PAPP-A)
According to international studies, combined first-trimester screening can identify approximately 75% of women who may later develop preterm preeclampsia before 37 weeks of pregnancy.
Preeclampsia screening at 11–13+6 weeks of pregnancy
Already in early pregnancy, during the early fetal anatomy ultrasound scan performed between 11 and 13+6 weeks, we assess not only fetal development but also the risk of preeclampsia and fetal growth restriction.
During this visit:
- The midwife measures your blood pressure using a standardized protocol
- A detailed medical and obstetric history is collected
- Blood tests are performed to assess placental markers
- Placental blood flow is evaluated using the uterine artery Doppler ultrasound
These examinations help estimate the risk of preterm preeclampsia, placental insufficiency, and fetal growth restriction.
Uterine artery Doppler examination and placental blood flow
Uterine artery Doppler examination is an important part of modern preeclampsia screening.
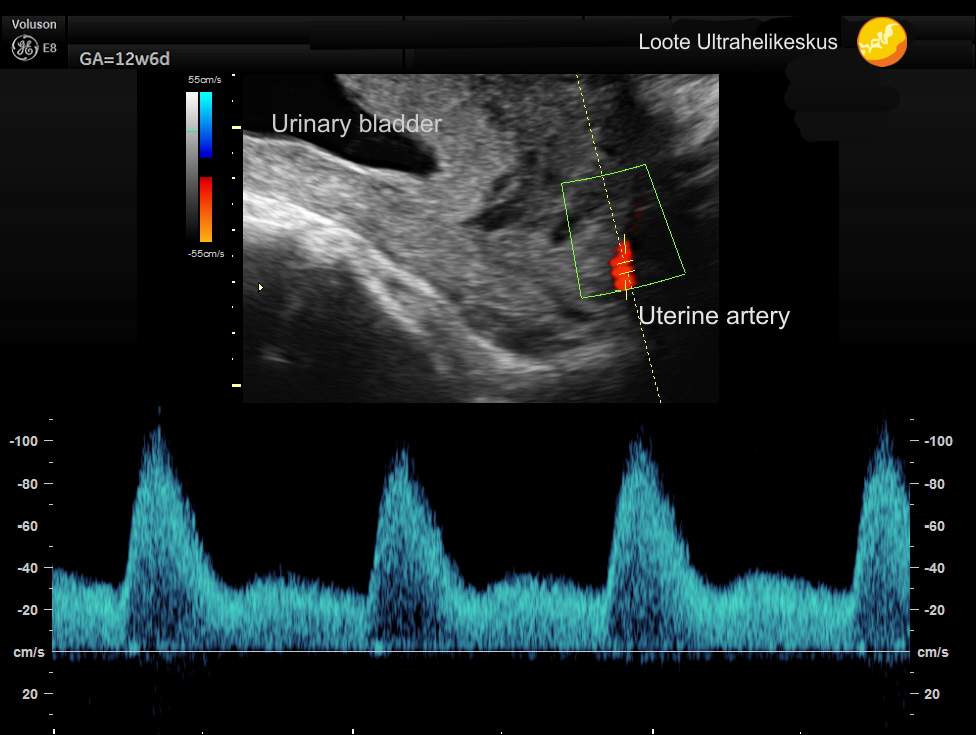
Figure. Uterine artery Doppler examination helps assess placental blood flow as well as the risk of preeclampsia and fetal growth restriction already in early pregnancy.
This examination allows us to assess placental blood flow already in early pregnancy. Changes in uterine artery blood flow may indicate an increased risk of:
- preeclampsia
- placental insufficiency
- fetal growth restriction
- preterm birth
During preeclampsia screening, blood flow in both uterine arteries is assessed, and specialized algorithms are used to calculate the individual risk of preterm preeclampsia.
At Loote Ultrahelikeskus, uterine artery Doppler examination is performed using a standardized methodology as part of a combined preeclampsia risk assessment.
If you belong to a higher-risk group, you may benefit from low-dose aspirin prophylaxis. Studies have shown that starting aspirin before 16 weeks of pregnancy may significantly reduce the risk of preterm preeclampsia.
Aspirin does not cure preeclampsia and cannot completely prevent the disease, but it may help reduce the risk of severe disease and delay its onset to a later stage of pregnancy.
Reassessment of preeclampsia risk in mid-pregnancy
For me, however, everything does not end with a single blood test or one ultrasound examination.
As pregnancy progresses, the most important question becomes how the baby is growing and how the placenta is functioning.
At around 20 weeks of pregnancy, we perform a detailed fetal anatomy scan. In addition to assessing fetal anatomy, we reassess uterine artery blood flow, placental function, and fetal growth.
This is a very important stage because it may be the first time signs of placental insufficiency begin to appear.
If the pregnancy requires closer monitoring, we create an individual follow-up plan.
Assessment of fetal growth and placental function in the third trimester
In the third trimester, one of the most important questions becomes fetal growth and well-being.
At approximately 32 weeks of pregnancy, the ultrasound assessment includes:
- fetal growth dynamics
- placental blood flow
- fetal circulation
- fetal wellbeing
If necessary, we also use computerized CTG monitoring, which provides an objective and accurate assessment of fetal condition.
In pregnancies affected by preeclampsia, we are not only concerned about whether the baby is growing too little. Sometimes fetal growth may still appear normal while the placental reserve is already decreasing. That is why we always evaluate the whole clinical picture.
Assessment of late-onset preeclampsia at 36 weeks
Toward the end of pregnancy, at approximately 36 weeks, we again assess fetal position, growth, placental function, and fetal well-being.
Based on this examination, it is possible to estimate the risk of late-onset preeclampsia and, if necessary, prepare an individual delivery management plan.
This is not a general recommendation, but a personalized plan based on your and your baby’s condition.
Together we discuss:
- When would it be safest to deliver
- Whether pregnancy can safely continue
- When induction of labor may become necessary
- And which mode of delivery may be safest
And perhaps most importantly, you do not go into labor without understanding what is happening.
You know how your baby is growing.
You know how the placenta is functioning.
And you know what the next step is.
You are not alone during this journey
At Loote Ultrahelikeskus, you are supported by a dedicated team, with the midwife playing a very important role. She measures blood pressure, collects blood tests, provides counseling, and helps ensure that any important changes are detected as early as possible.
Our goal is not to perform more examinations, but to perform the right examinations at the right time and to support you throughout your pregnancy journey.
Most women with an increased risk of preeclampsia go on to deliver a healthy baby. The most important thing is that the risk is recognized early and the pregnancy is monitored carefully and scientifically.
Preeclampsia risk calculator during pregnancy: Preeclampsia Risk Calculator
Dr Marek Šois
Obstetrician-Gynecologist, specialized in Fetal Medicine