The Fetal Ultrasound Center offers pre-eclampsia screening to pregnant women
Every expectant mother wants her pregnancy to be a happy time. However, the joy can be shadowed by the fear of preeclampsia.
What is preeclampsia?
Preeclampsia is a potentially life-threatening condition that affects many organs during a pregnancy and is characterised by an increased maternal arterial blood pressure and the appearance of protein in the urine or, in the absence of the latter, malfunctioning of other organs. This can affect both you and your unborn baby. If the risk of preeclampsia is known in advance, it can be prevented.
How common is preeclampsia?
In most women, pregnancy takes a normal course. However, preeclampsia is a relatively common condition during pregnancy, occurring in Estonia in two pregnant women out of a hundred.
When does preeclampsia occur?
Preeclampsia occurs after the 20th week of pregnancy or up to six weeks after delivery. Preeclampsia is more common between the 32nd and 36th weeks of pregnancy. The earlier the condition develops during pregnancy, the more severe its course, and the more dangerous it is to the mother and child.
What causes preeclampsia?
The precise causes of pre-eclampsia are not known, but it is believed that at the centre of origin of the condition is a placental attachment disorder in the uterus, which results in poor contact between the foetal and maternal circulatory system. However, the fast-developing foetus requires oxygen and nutrients from the maternal circulatory system for growth. If the developing placenta develops oxygen deficiency, toxic substances are released into the maternal bloodstream that damage the maternal vascular mucous tissue. This causes systemic damage to the internal organs of the mother. The child must be delivered in order to save the mother and the child. However, if this happens at a very early stage, the child is not yet ready for extrauterine life.
How does this affect me?
In most cases, there is a mild form of the condition that occurs at the end of pregnancy, the prognosis of which is good. But sometimes, preeclampsia can become more severe very rapidly and endanger the mother's life and health. Preeclampsia also has prolonged effects on the health of a woman as it doubles the occurrence of cardiovascular diseases in later life. Most women with preeclampsia are taken to the hospital and often have to have their children delivered prematurely. If the mother or child's health is in danger, the delivery will be induced or a Caesarean section carried out.
How does this affect my child?
Most children remain healthy, even when their mother has severe preeclampsia. But sometimes, the mother's preeclampsia may endanger the life and health of both the foetus and the newborn. The occurrence of preeclampsia in the mother doubles the risk of cerebral palsy or brain damage of the surviving children, which results in physical and, sometimes, mental retardation. The surviving children also frequently have more cardiovascular diseases, weight issues, and diabetes later in life. In the case of preeclampsia, there is not enough oxygen and nutrients for the growth of the foetus and there is intrauterine stunting. Since the only treatment for preeclampsia is delivery, pregnancy must sometimes be terminated prematurely. Before the 34th week of pregnancy, the foetal lungs are not yet fully developed and the pregnant woman is given steroid injections to help improve the foetal lungs.
How do I recognise preeclampsia?
Unfortunately, in most women, the signs of the condition only appear in the final stages of the disorder.
- Persistent headache, which does not respond well to painkillers
- Severe nausea and vomiting
- Vision disturbances, murmuring in the ears
- Subcostal pain in the right side
- Feeling out of breath, shortness of breath
- Infrequent need to urinate (less than 500 ml per day)
- Swelling of hands, face, and eyelids
- Rapid weight gain (over 1 kg in one week)
If the symptoms listed above occur, contact your midwife, gynaecologist or hospital doctor on duty.
Am I at risk?
Although preeclampsia may occur in all pregnant women, some women are more at risk than others.
You are at a higher risk if
- This is your first pregnancy;
- You had preeclampsia during the previous pregnancy;
- Your mother or sister has had pre-eclampsia;
- Your body mass index is 35 kg/m2 or more;
- You are 40 years of age or older;
- The time between childbirths has been more than 10 years;
- You are expecting multiple children;
- You became pregnant via artificial fertilisation treatment;
- You have a medical condition, such as hypertension, kidney problems, lupus, diabetes;
- You had diabetes during this pregnancy.
At what gestational stage is the screening performed?
Screening for preeclampsia can be performed in all three trimesters.
- In the 11th-13th+6 gestational week of the first trimester (within the OSCAR test)
- In the 19th-21st+6 gestational week of the second trimester (within the anatomical screening of a foetus)
- In the 34th-36th gestational week of the third trimester (within the foetal growth and wellbeing survey)
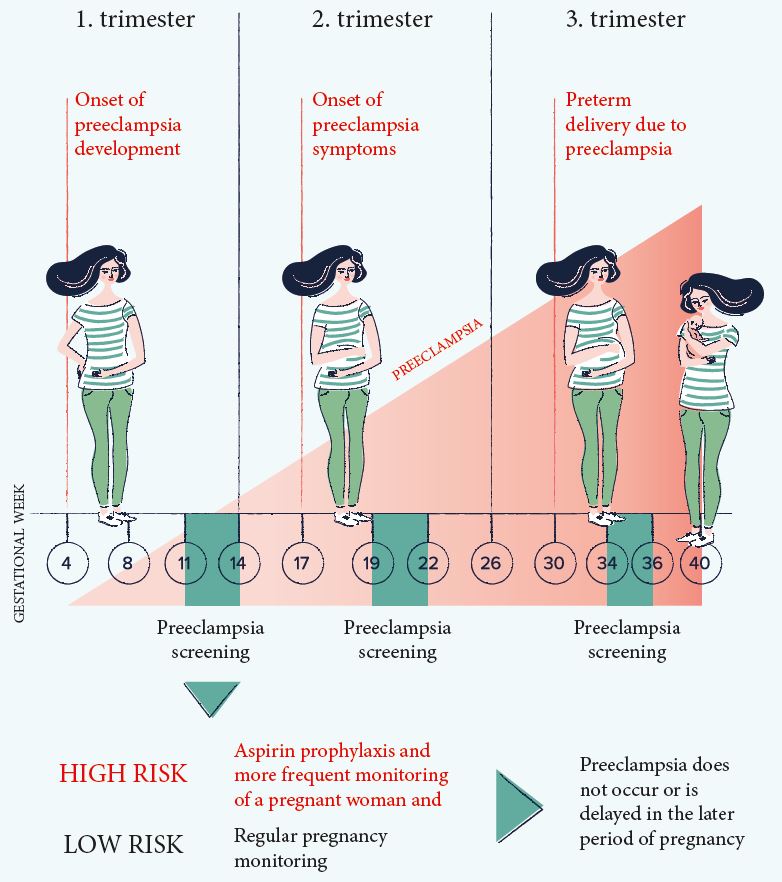
The three-stage preeclampsia screening provides the opportunity to prevent the onset of preeclampsia or to delay it to a later period of pregnancy.
How reliable is preeclampsia screening?
With the OSCAR test in the I. trimester, 76% accuracy could be reached in the identification of women at risk who may develop early preeclampsia before the 37th week of pregnancy. In the case of a pregnancy with twins, it is possible to identify all women who may develop early preeclampsia before the 37th week.
During the foetal anatomical screening in the II. trimester, it is possible to identify women at risk who may develop early preeclampsia before the 37th week with 85% accuracy.
During the ultrasonic examination of foetal growth and wellbeing in the III. semester, it is possible to identify women at risk who may develop the late-onset preeclampsia after the 37th week with 85% accuracy.
Why should I assess my risk of preeclampsia?
During the OSCAR test in the I. trimester, the assessment of the risk of development of early preeclampsia is best, and women at risk benefit from the preeclampsia-preventing effect of aspirin. Studies have shown that at low doses, aspirin intake prior to the 16th week of pregnancy reduces the onset of early preeclampsia in 62% of cases, which may require delivery before the 37th week of pregnancy. Therefore, it is recommended that women with a higher risk should take 150 milligrams of aspirin once a day in the evenings up to the 36th week of pregnancy. The objective of the treatment of women with a high risk of preeclampsia is to prevent the development of preeclampsia or to delay its onset in a later pregnancy period if the child is mature enough to be born.
During the foetal anatomical screening of the II. trimester, the risk of preeclampsia obtained during the OSCAR test may be reassessed or preeclampsia screening may be recommended for women whose preeclampsia risk was not assessed during the OSCAR test.
During the ultrasonic examination of foetal growth and wellbeing in the III. trimester, late preeclampsia can be assessed. This is very important as 75% of preeclampsia cases occur after the 37th week of pregnancy. This provides an opportunity to monitor women with a higher risk of preeclampsia more frequently and to detect the condition in a timely manner and prepare the child's lungs for the forthcoming birth.
How is preeclampsia screened?
Preeclampsia screening consists of a nurse's check-up and a gynaecologist's ultrasonic examination. A nurse questions the pregnant woman, measures her blood pressure, height and weight, and conducts a blood test. A gynaecologist carries out an ultrasonic examination of a foetus and measures the blood flow indexes of uterine arteries supplying the placenta. By combining the values of hormones assigned from a blood test with the preeclampsia risk factors, blood pressure values, body mass index and blood flow indexes of uterine arteries of a pregnant woman, the gynaecologist calculates a woman's individual early or late risk of preeclampsia using a special computer program.
- The risk of preeclampsia can be assessed within one day.
- The risk of preeclampsia can also be assessed in women who are expecting twins.
Preeclampsia screening gives you a sense of reassurance
Most of the women participating in the preeclampsia screening belong to a low-risk group. In the case of an increased risk, the triple-stage preeclampsia screening gives you the opportunity, if necessary, to prevent the onset of preeclampsia, or to delay it to a later period of pregnancy. A sense of reassurance really necessary for you results from the reduction of the risk of preeclampsia and by careful, research-based monitoring of you and your child's state of health. In this way the child can safely be born when s/he is ready, and you can rejoice in a healthy child.